
LifeSiteNews is on the cutting edge of life and family news reporting. Support our Summer Campaign by giving a gift of support today: give.lifesitenews.com
(Paul Alexander) – If our immune response is subverted and damaged by these COVID injections, as they have been with repeat boosting, then we run the risk of this pandemic going on for 100 years with infectious variant after infectious variant, and potentially a lethal virulent one that could devastate humanity.
COVID will never ever end, and though I am beginning to sound conspiratorial by saying so, I do think people like Fauci and Pfizer’s CEO Albert Bourla cannot be so foolish or inept as they appear. This situation is being managed deliberately at some level. We see that sub-variant after sub-variant is posing an escalating infection risk in those vaccinated (whether mRNA or adenoviral vector injections). It seems like this will go on in perpetuity; long-term, with no end in sight.
Mass vaccination has made things devastatingly worse. We told them to stop, over and over: one should never ever mass vaccinate while there is a circulating pathogen.
We devastatingly underestimated the evolutionary capacity of the COVID virus to evolve and adapt to the sub-optimal immune pressure on the spike. We have underestimated the viral-host immune ecosystem, the complex interplay. One cannot study or debate or assess the devastation of these fraudulent COVID injections without considering the virus-host ecosystem. It is not simply the properties intrinsic to the virus that are causing the immune escape and infection in the vaccinated. Individuals such as Fauci and Bourla and Njoo and Tam and Walensky must not exclude the definitive impact of the non-neutralizing antibodies on the target antigen.
Moreover, we have to consider that recent omicron sub-variants such as BA.4 and BA.5 may be completely novel COVID viruses and not necessarily variants of the omicron. They are evading immunity on such a large scale that we need to consider this, as this then will limit natural immunity, yet prior infection and recovery may still offer some level of protection. We need to quickly consider and assess this. The key issue as we have said day one, is that these sub-optimal flawed failed fraud of COVID vaccines is driving this. This is why we called, one year now, to stop these COVID vaccines immediately.
I will repeat what Geert Vanden Bossche is developing and saying: that currently, while sub-optimal vaccine induced antibodies to omicron enhance infection in the upper respiratory tract (URT), and at the same time reduce severity in the lower respiratory tract (LRT) – by blocking transfection or transmission of infection from infected cells to non-infected cells in the LRT – this ‘nature’s gift’ we thought we had will not go on much longer.
Severe disease is coming soon in the LRT, deep inside the lungs. The very same vaccinal antibodies to omicron that are blocking severe disease in the LRT, are subjected to sub-optimal immune pressure that will drive variants to overcome this pressure. Geert explains (based on published research) that these non-neutralizing antibodies in the LRT are linked to the formation of syncytia that is correlated to severe illness.
I will say it again (standing on shoulders of GVB): it is the mass vaccination in a pandemic, as we did here in February 2021, using a non-sterilizing vaccine (vaccinal antibodies that do not neutralize or sterilize the virus where the virus became largely resistant to the vaccinal antibodies) that pressures the spike (infectiousness of the virus), as there is massive infectious pressure.
This mounting ‘immature’ host immune pressure on the spike via a non-neutralizing injection is the key devastating issue. This drives selection pressure to select the fittest and most infectious variants that will become enriched in the environment and proliferate and be the new dominate variant/clade/sub-variant e.g. Omicron BA.5.
There is consequent antibody-dependent enhancement of infection (ADEI), where the vaccinated gets massively infected post vaccine, and original antigenic sin (OAS) that I renamed mortal antigenic sin (MAS) as the initial imprinting, priming, exposure prejudices the immune response life-long to the initial antigen/exposure or similar. The recall antibodies are to the initial Wuhan legacy strain and not the current omicron clade.
Yahi et al. has presented intriguing research showing that the vaccinal antibodies bind to the virus’s spike receptor binding domain and/or N-terminal domain (binding sites) yet cannot sterilize the virus (eliminate it, stopping infection or transmission). This binding was shown to actually facilitate and enhance infection in the vaccinated (ADEI).
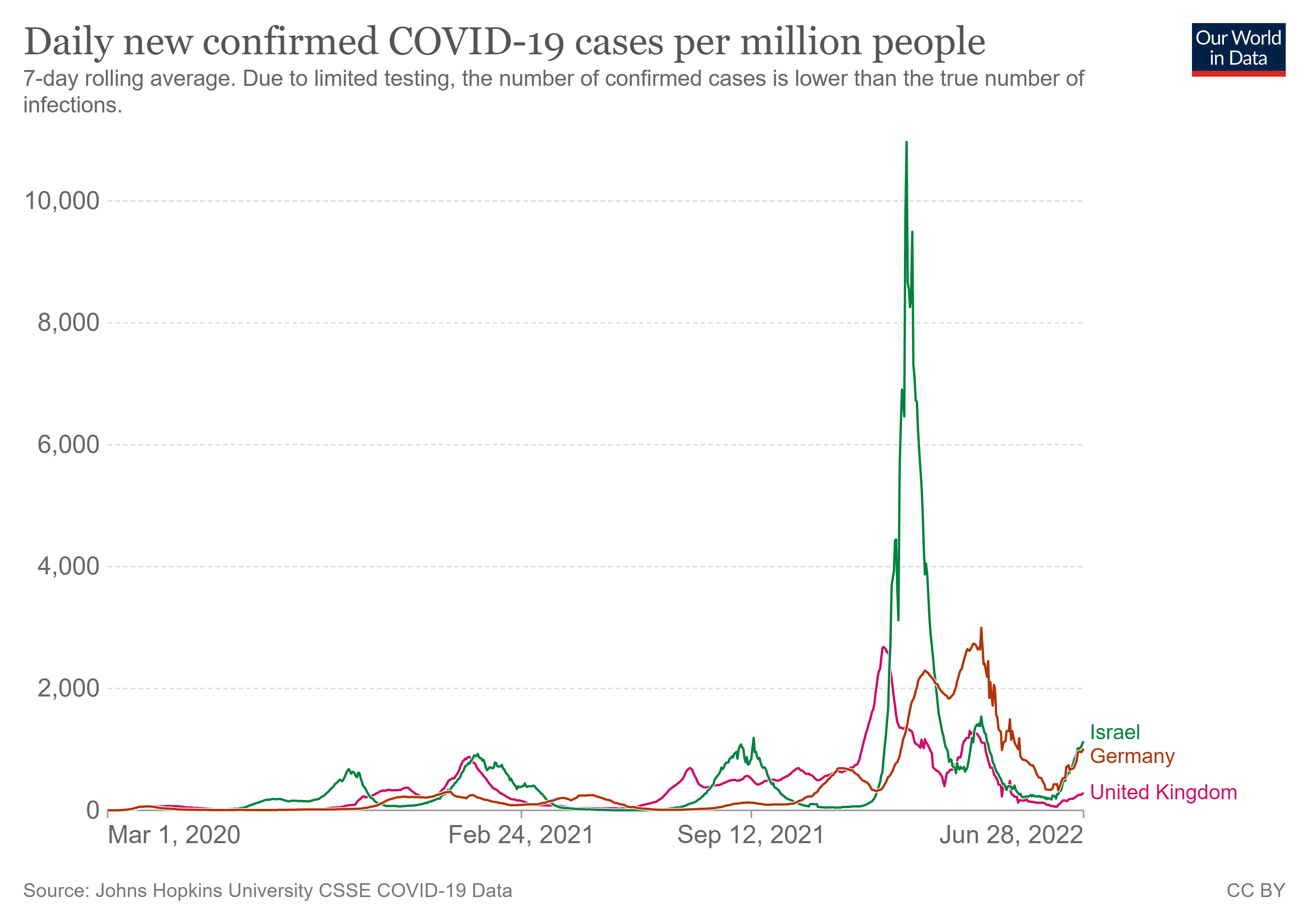
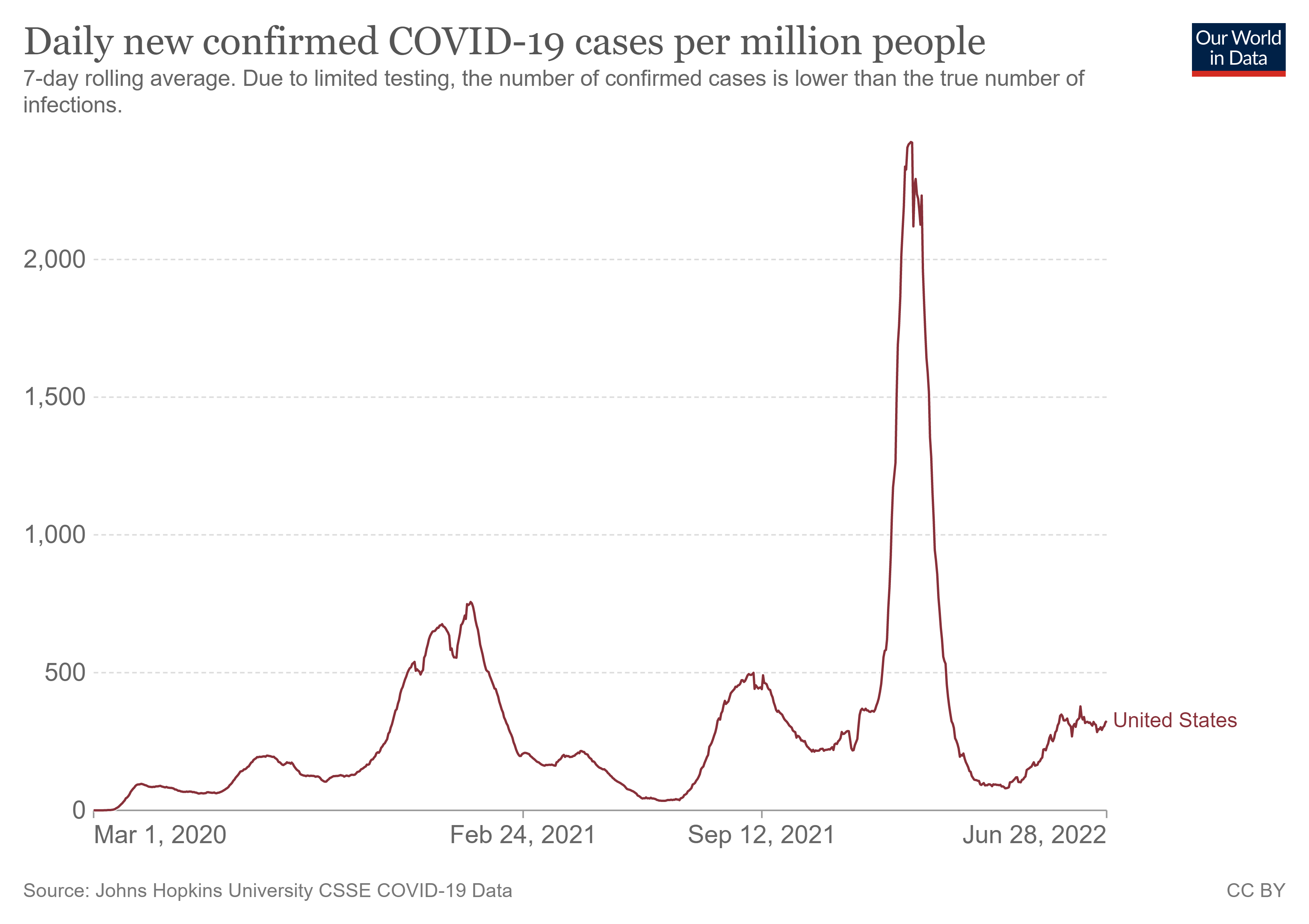
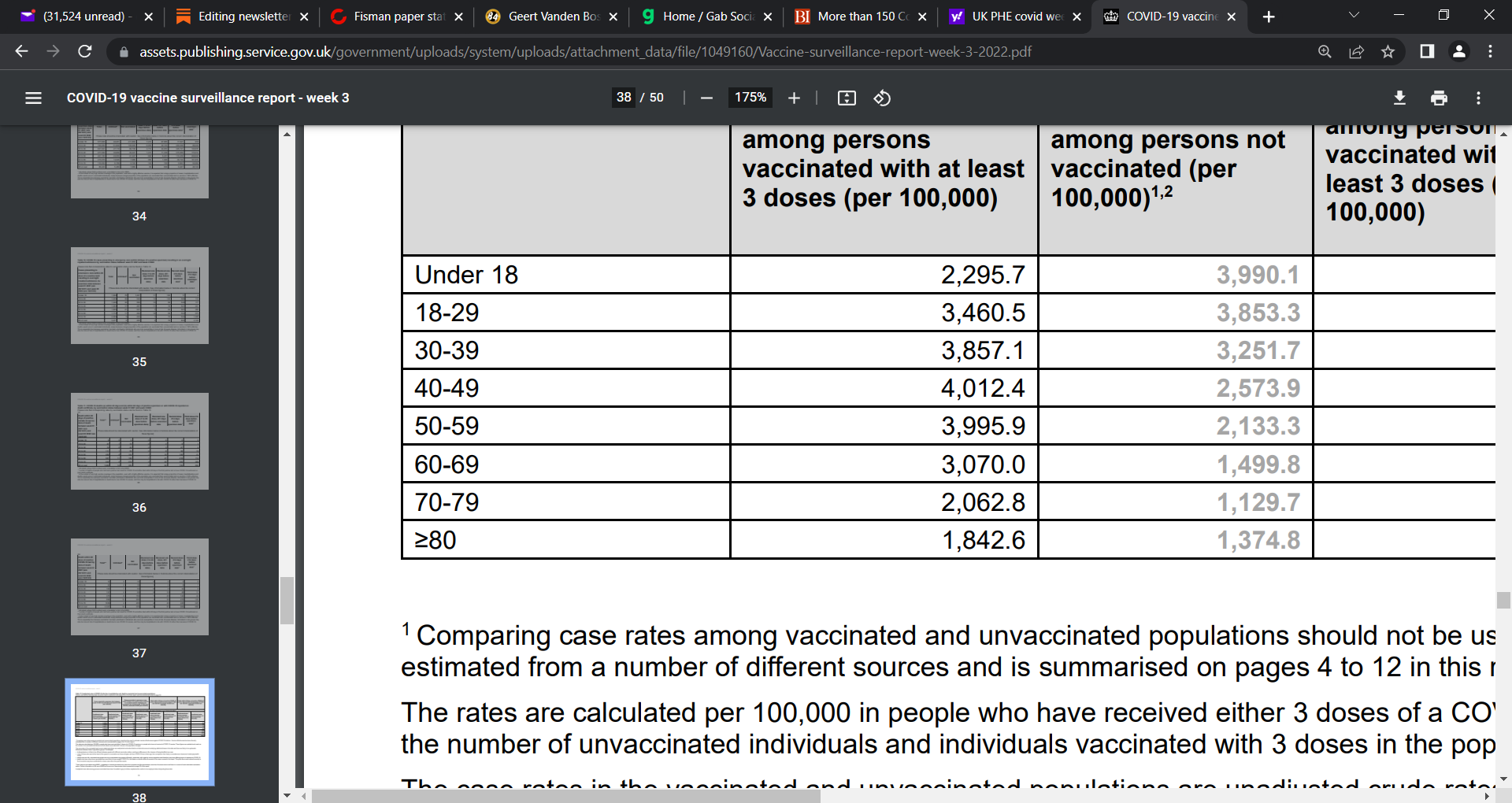
Updated case graphs:
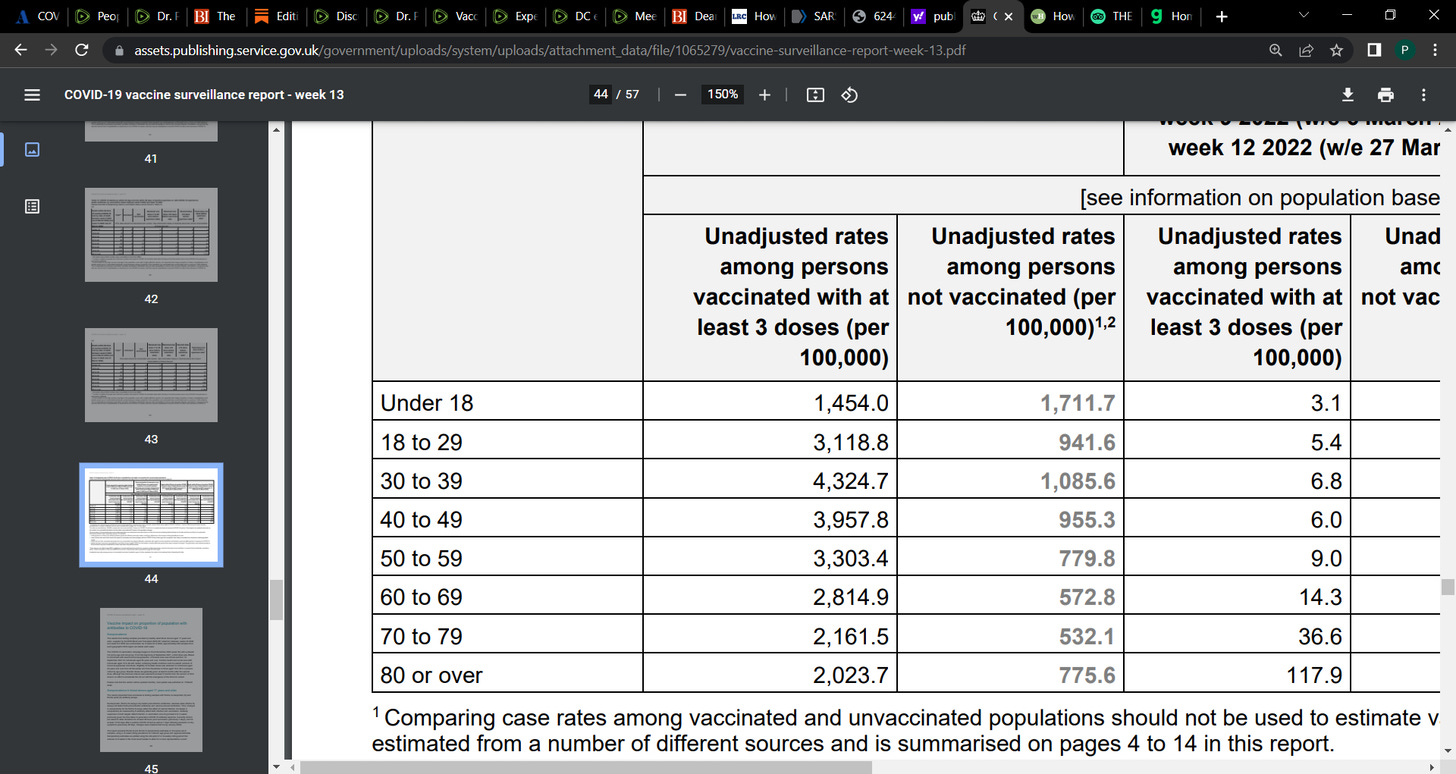
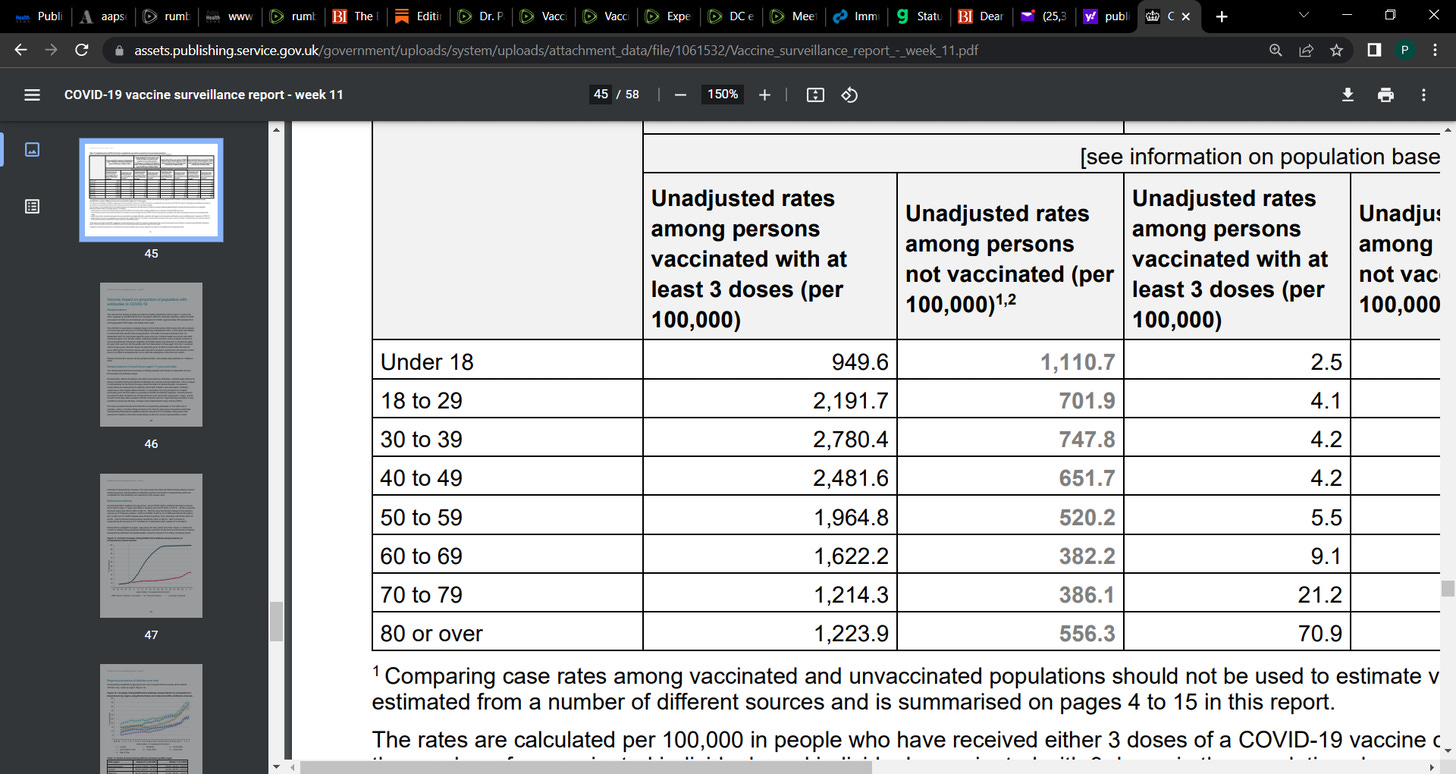
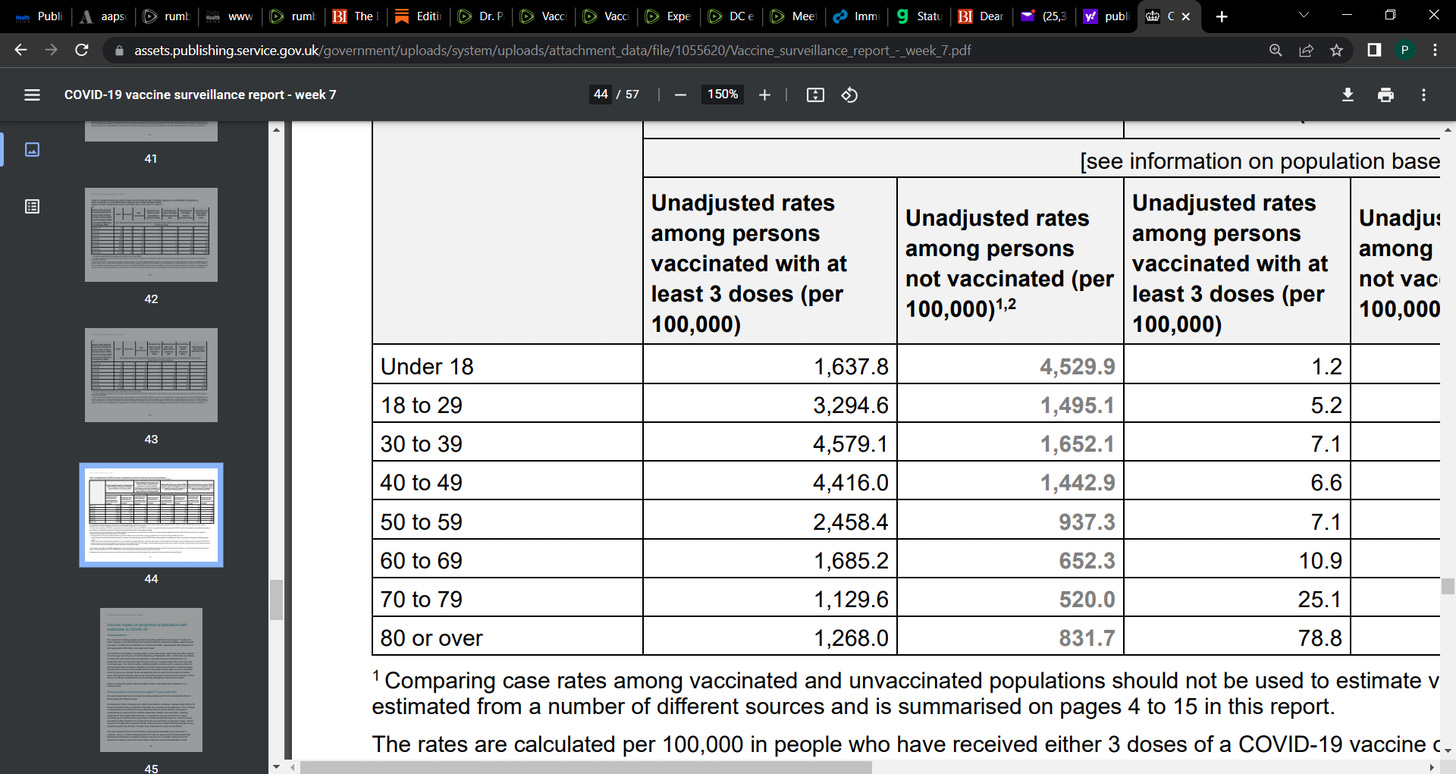
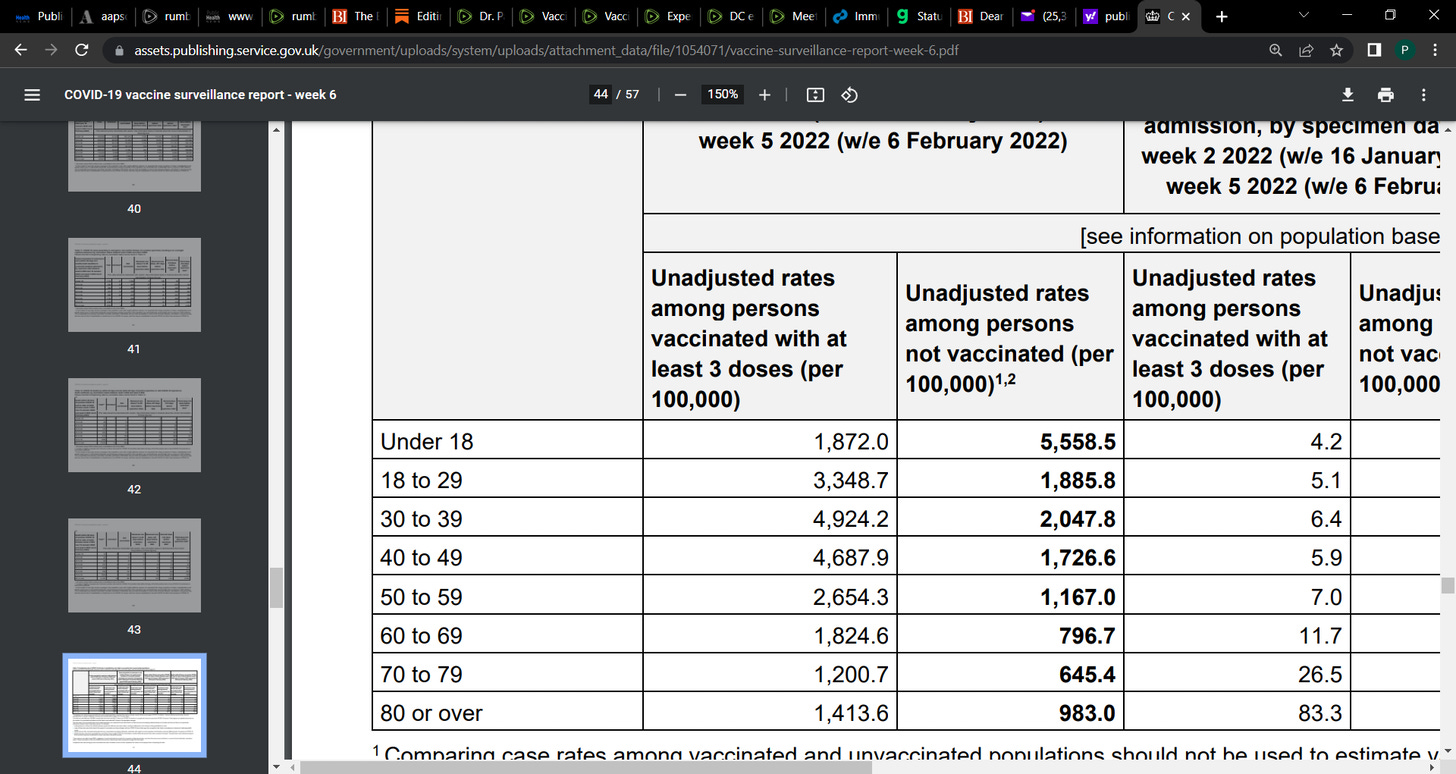
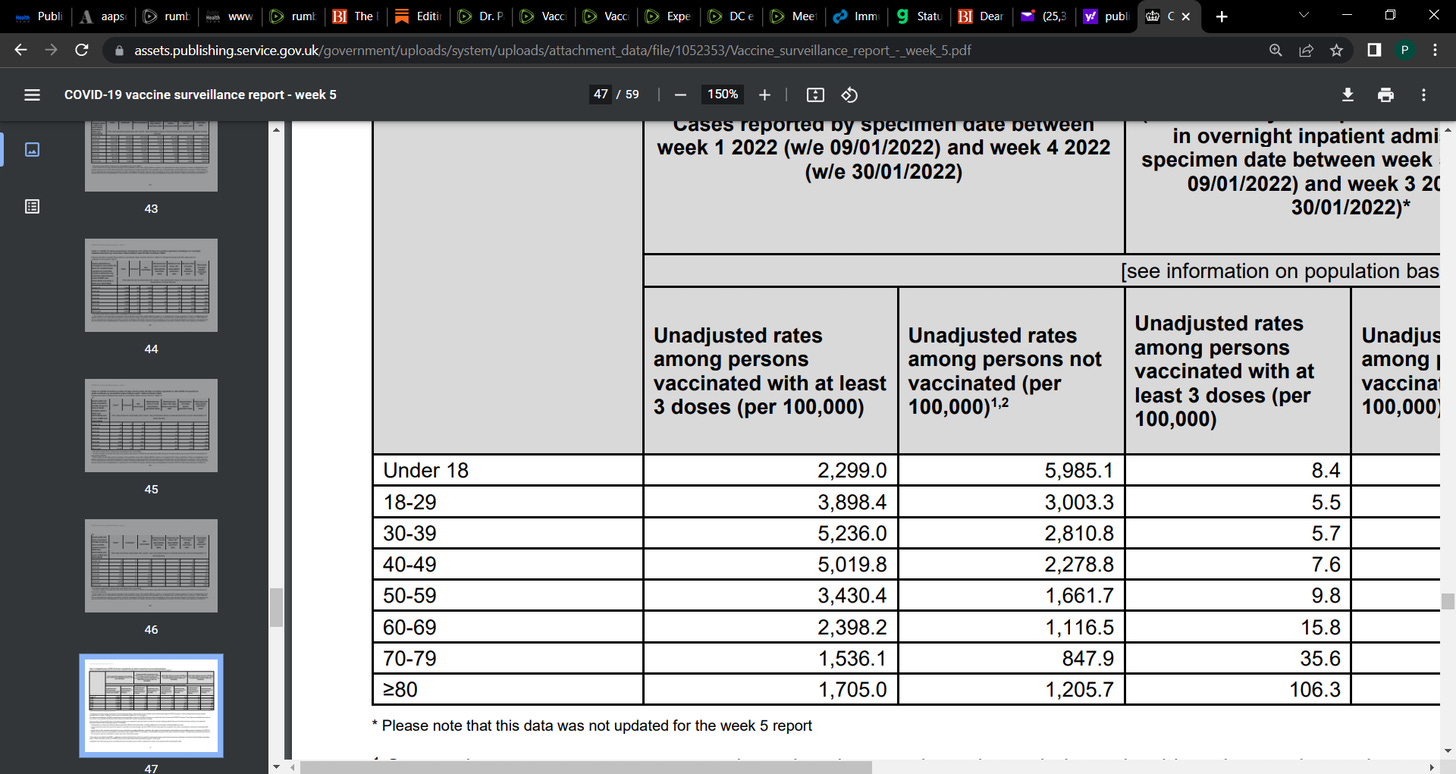
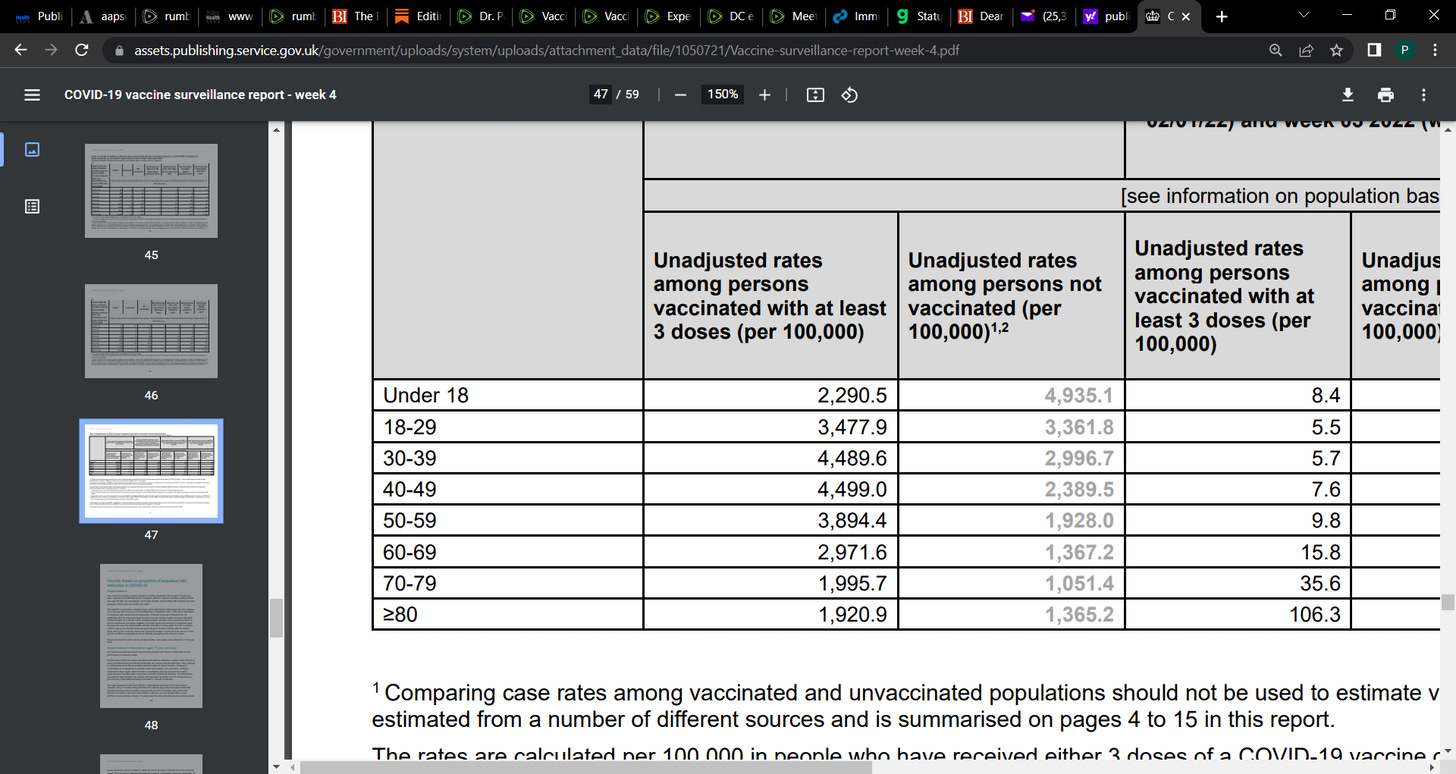
I have included the case data for UK up to week 13 this year (below), March 2022, in which the data was so bad, that the UK government stopped reporting the double and boosted vaccinated persons. The data was catastrophic showing how vulnerable the vaccinated were.
COVID-19 vaccine surveillance report Week 13 31 March 2022
Week 13 infection:
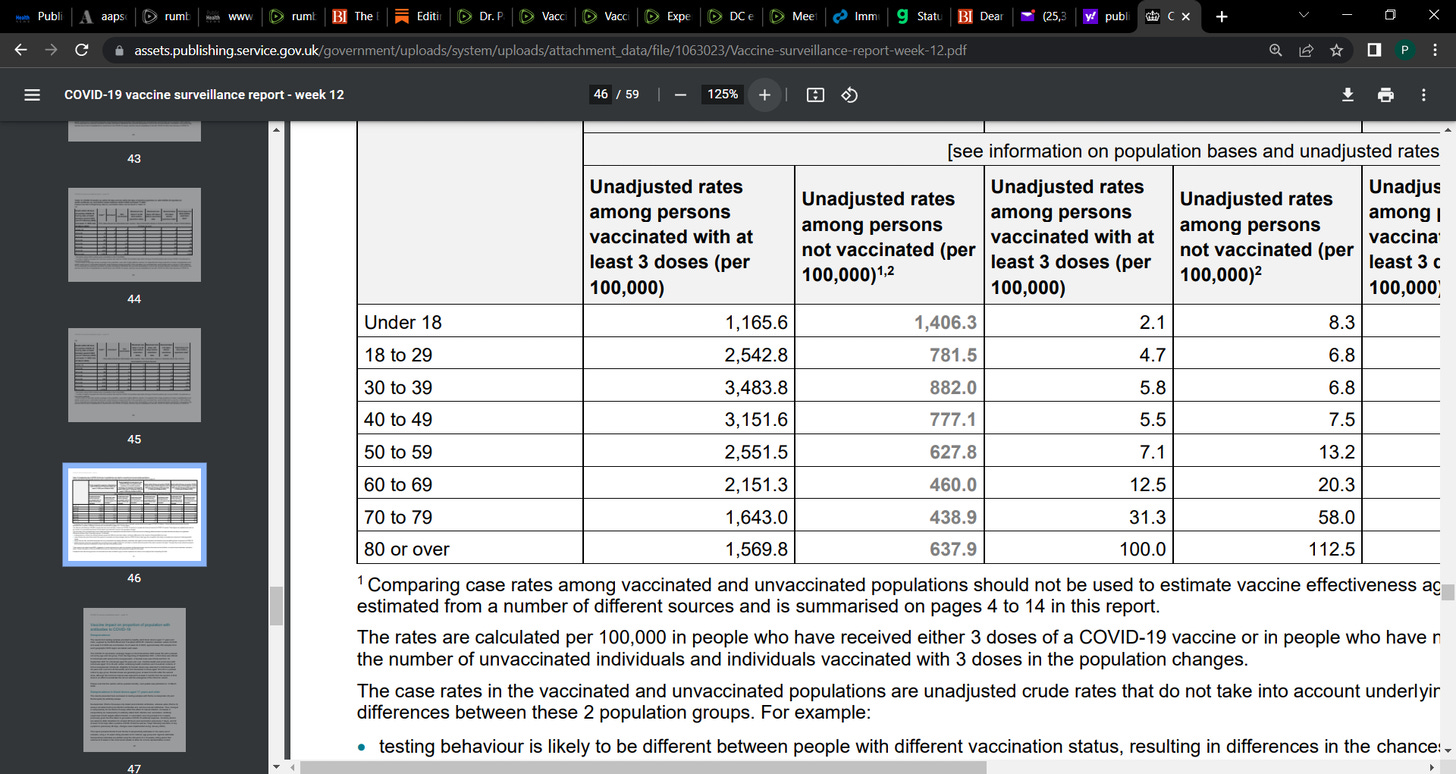
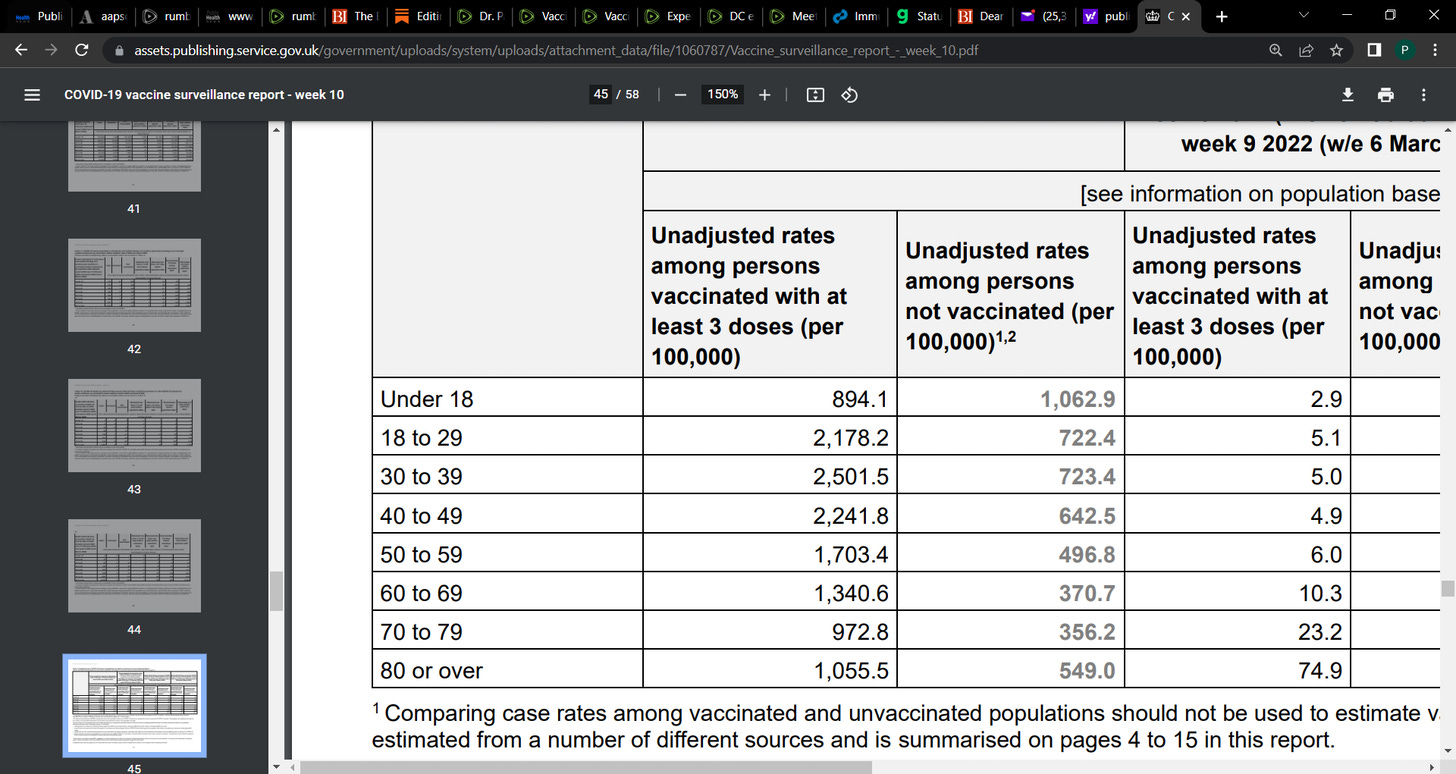
Week 10 infections
Reprinted with permission from Paul Alexander